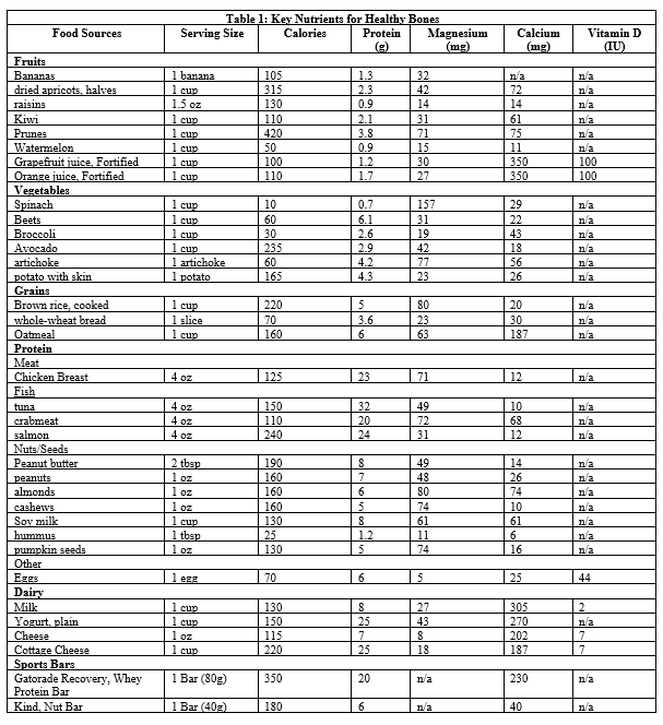
 By Taylor Hoeg, Graduate Nutrition Student Bone Density or Bone Mineral Density (BMD) is a measure of how much bone mineral is in bone tissue. Bone is in a constant state of remodeling or breaking down. Low BMD is happening when more bone is breaking down than building. BMD is especially important for athletes because of its effects on short- and long-term performance. In the short-term, athletes with low BMD are at higher risk for stress and general bone fractures. Low BMD is a condition that weakens bone and with lower structural matrix of the bone, bone is frail and easier to fracture from repetitive use or impact from usual sports training. The long-term consequence of low BMD for athletes is the much higher risk of developing osteopenia or osteoporosis. These conditions, most often thought of with elderly, can also occur in young athletes with chronic low BMD. These conditions are characterized by greater bone fragility and increased risk of fracture (Kerr & Enette, 2015), again painting the picture that weak, frail, and thin bones increase risk of injury that can derail optimal training, competition, and athletic performance. The advantage for athletes is that exercise is known to increase bone health and density, in other words, exercise builds stronger bones (Goolsby & Boniquit, 2017). However, exercise alone cannot fully protect bone health. Poor nutrition increases an athlete’s risk for low bone density, putting the athlete at risk for compromised performance, injury and delayed recovery. Sport, gender, and diet all affect BMD in athletes. Activities and sports that involve impact and weight-bearing promote bone mineralization, which leads to stronger and denser bones. Weight-bearing exercise and sports that build bone include strength training and conditioning, baseball, softball, soccer, wrestling, tennis, and volleyball. Non-impact sports, although important for overall health and wellness have less effect on bone building, such as swimming, water polo, and cycling (Tenforde & Fredericson, 2011). Physiologically, women tend to have smaller and thinner bones than men, thus simply, women have increased risk of developing low BMD. Complicating the issue for women, is that low estrogen levels which commonly occurs in female athletes leads to amenorrhea which then contributes to bone breakdown, low BMD, and very high risk for fracture. Diet plays a critical and essential role in healthy BMD. Athletes need optimal nutrition. Eating a diet with enough calories and choosing a variety of foods can provide the essential bone building nutrients, such as protein, calcium, vitamin D, and magnesium. When diet is inadequate, both male and female athletes can experience Relative Energy Deficiency in Sports (RED-S). RED-S develops when athletes do not consume enough calories to meet their needs for exercise and health. Low calorie intake, also referred to as low energy intake, may or may not be a purposeful restriction of calories, but more so a consequence of extensive exercise training and not eating enough to match the athletes refueling needs. For example, a busy student athlete whose schedule involves attending classes and multiple training and practice sessions may simply not eat enough during the day to meet all his/her calorie needs. Student athletes may not have time for meals if they are rushing from practice to class across campus (and vice versa), class times overlap meal times, they don’t have time to go to dining services or home for meals, don’t bring food with them to eat throughout the day, or don’t have the financial means to purchase enough food. However, low calorie intake is also, unfortunately, very commonly a result of a true eating disorder among athletes, and should not be overlooked by athletes, coaches, or trainers. Adequate caloric/energy intake ensures athletes maintain lean body mass, fat mass, and female athletes have a regular menstrual cycle, all of which contribute to building strong bones and a high BMD (Kerr & Enette, 2015). Calorie needs are determined for each individual athletes based on a number of factors including: age, gender, height, weight, and level of physical activity (Estimated Calorie Needs per Day, by Age, Sex, and Physical Activity Level, 2015). Below, is a link to a calorie calculator, which is a good starting point for determining your calorie needs. BUT, a word of caution, this is a really basic calculation and not at all individualized to YOU. https://www.mayoclinic.org/healthy-lifestyle/weight-loss/in-depth/calorie-calculator/itt-20402304 Protein makes up 50% of the bone, and bone is constantly remodeling, therefore, an adequate daily supply of protein is required for bone health (Wallace, 2019). Athletes need more protein due to training and competition. Protein recommendations for most athletes is 1.2-1.7g/kg/d. The goal is to choose high quality protein foods, from a variety of animal and/or plant sources, that also provide needed calories, vitamins, and minerals. See Table 1 below for protein suggestions. Calcium is the main mineral stored in bones and teeth and is vital for muscle contraction (Calcium, 2019). Adequate levels of calcium are essential for building strong bones and maintaining high BMD. Current evidence suggests 1,500 mg per day of calcium is protective against stress fracture and supports healthy bone density in athletes (Kerr & Enette, 2015). It is always recommended to find ways to boost calcium in your diet from food sources. Dietary food sources of calcium are often better absorbed, and provide other essential nutrients and calories, as well. It is important to note, calcium cannot be absorbed in larger doses than 500 mg at a time, therefore choosing calcium foods throughout the day is the best approach to meeting your calcium needs. Calcium supplementation may be warranted in some cases, however, consultation with a physician and/or Registered Dietitian Nutritionist are often helpful in determining whether supplementation is needed. When supplementation is needed, it is always in conjunction with improving dietary intake of calcium, as well. Should a supplement be needed, distributing 3 separate doses across the day would be needed to reach the 1500 mg/d recommendation. It’s also important to consider the type of calcium used in the supplement, as calcium is better absorbed in an acidic environment. For example, calcium citrate is better absorbed than calcium carbonate. A word of caution when it comes to supplements, over-supplementation of calcium can cause hypercalcemia, which can cause fatigue, nausea, vomiting, constipation, back pain, and forgetfulness (Kerr & Enette, 2015). More is not usually better when it comes to supplements, always try FOOD FIRST! See Table 1 below for a list of high calcium foods. Vitamin D aids in the absorption and regulation of calcium. Adequate levels of Vitamin D are essential for maintaining high BMD and preventing bone injury. It is the combination of Vit D and calcium that strongly influence bone mineralization. Inadequate Vit D and/or calcium lead to poor bone status and increased risk for injury and poor performance. The primary source of Vitamin D is from sun exposure and absorption through the skin. As compared to calcium, fewer Vit D food sources are available. Since meeting recommendations for Vit D primarily involves exposure to sun, all athletes whose sport involves most of their time indoors are at risk for poor Vit D status. Which includes many student athletes, who also spend a significant amount of time indoors while in class. Athletes with darker skin are also at risk for poor Vit D status because the darker skin pigment interferes with Vit D absorption. Thus, a large proportion of the athlete population is at risk for poor Vit D status and would greatly benefit from sun exposure and increasing Vit D from foods. Recommended dietary allowance (RDA) for Vitamin D is 600 IU for adults. For athletes who train exclusively indoors and do not get sufficient daily sun exposure, the Endocrine society of USA recommends 1,500-2,000 IU (Kerr & Enette, 2015). This recommendation is more than double the recommendation for average adults and reinforces the message that athletes have much higher Vit D needs to support healthy bones for optimal training and peak performance. See Table 1 below for dietary sources of Vitamin D. Last, magnesium plays a critical role in the structural development of bone. Insufficient dietary magnesium contributes to osteopenia or osteoporosis by weakening bone cells, decrease activity of the parathyroid hormone and increased inflammation (Castiglioni, Cazzaniga, Albisetti, & Maier, 2013). The recommended intake of magnesium for athletes is 500 to 800 mg daily (Seelig, 1980) and magnesium can be found in a wide variety of different foods. See Table 1 below. Here’s the bottom line: athletes need to nourish to flourish! To prevent injury, reach your peak performance and have a successful sports career, you need to eat enough food and a variety of foods with protein, calcium, vitamin D, and magnesium to build and maintain strong bones. Go COUGARS References
0 Comments
Leave a Reply. |
Contributing AuthorsSIUE Nutrition and Dietetics Graduate Students See More Helpful Nutrition Tips Here
April 2023
Categories |


 RSS Feed
RSS Feed
